
- Assessment is Critical: Utilizing the six ASAM dimensions ensures that placement in inpatient addiction treatment centers is based on clinical necessity rather than guesswork.
- Medical Safety First: Severe withdrawal risks and complex co-occurring conditions are primary indicators for 24-hour medical monitoring.
- Environment Matters: A chaotic or unsupportive home environment is a significant factor in recommending residential care over outpatient options.
- Duration Impacts Outcome: Research consistently supports 90-day programs for better long-term stability compared to shorter stays.
- Plan for Aftercare: A structured step-down pathway is essential for maintaining gains made during residential treatment.
Understanding Residential Care Intensity
How Multidimensional Assessment Guides Placement
Start with this tool: a quick readiness checklist. Ask yourself—does the individual show severe withdrawal risk, unstable medical or psychiatric conditions, low motivation for recovery, or a home environment that could undermine progress? If you’re nodding yes to more than one, a multidimensional assessment is likely needed.
A multidimensional assessment is a structured evaluation tool that looks at several key areas of a person’s life and health to decide what level of care will offer the best chance of success. The gold standard for this is the ASAM Criteria, which reviews six distinct dimensions—including withdrawal potential, biomedical needs, emotional complications, motivation, relapse risk, and recovery environment—to guide placement decisions2.
This approach works best when you’re facing complex cases. For example, if someone presents with both substance use and unmanaged depression, the assessment helps clarify whether outpatient support is enough or if inpatient addiction treatment centers offer the safety net required.
According to national guidelines, using a multidimensional assessment leads to more accurate placements, which reduces premature discharge and increases treatment retention3. Time investment for a full ASAM-based assessment usually ranges from 60 to 90 minutes and calls for a multidisciplinary team—think medical providers, therapists, and case managers all contributing their insights. Every step forward counts here: a careful assessment means you’re setting up the person in your care for the best possible outcome.
Up next: you’ll look closer at the six ASAM dimensions and how each uniquely influences the decision to recommend residential care.
The Six ASAM Dimensions That Matter Most
Let’s use this practical tool: a six-point ASAM decision worksheet. For each dimension below, rate the individual’s risk as low, moderate, or high. A higher rating in multiple areas points toward recommending more intensive care settings, such as inpatient addiction treatment centers.

- Acute Intoxication and Withdrawal Potential: Does the person face risk of severe withdrawal or intoxication that could require urgent intervention? High scores here indicate the need for close medical monitoring.
- Biomedical Conditions and Complications: Are there ongoing physical health issues—like heart disease, diabetes, or chronic pain—that could complicate recovery? If these are present and unmanaged, residential care offers the needed support.
- Emotional, Behavioral, or Cognitive Conditions: Consider the impact of mental health conditions such as depression, anxiety, or trauma histories. When symptoms are severe or unstable, residential settings provide structure and safety2.
- Readiness to Change: Assess motivation and willingness to engage. If motivation is low or ambivalent, a higher level of support can nurture momentum for change.
- Relapse, Continued Use, or Continued Problem Potential: Count recent relapses or persistent use. High risk in this area signals the benefit of an immersive environment free from triggers.
- Recovery/Living Environment: Is the person’s home environment safe and supportive? If not, the structure and supervision of inpatient addiction treatment centers may be essential3.
This approach is ideal for those with multiple risks that can’t be safely managed in outpatient care. Yes, this is challenging, and that’s okay—each careful rating brings you closer to the right care plan. Next, you’ll see how these same dimensions guide the call for 24-hour medical support.
Clinical Indicators for 24-Hour Medical Care
Severe Withdrawal Syndromes Requiring Monitoring
Use this quick triage checklist to identify when inpatient addiction treatment centers are the safest option for withdrawal management:
- Is the person at risk for severe withdrawal symptoms (such as seizures, hallucinations, or unstable vital signs)?
- Have they previously experienced complicated withdrawal?
- Are there co-existing medical or psychiatric issues that could escalate during withdrawal?
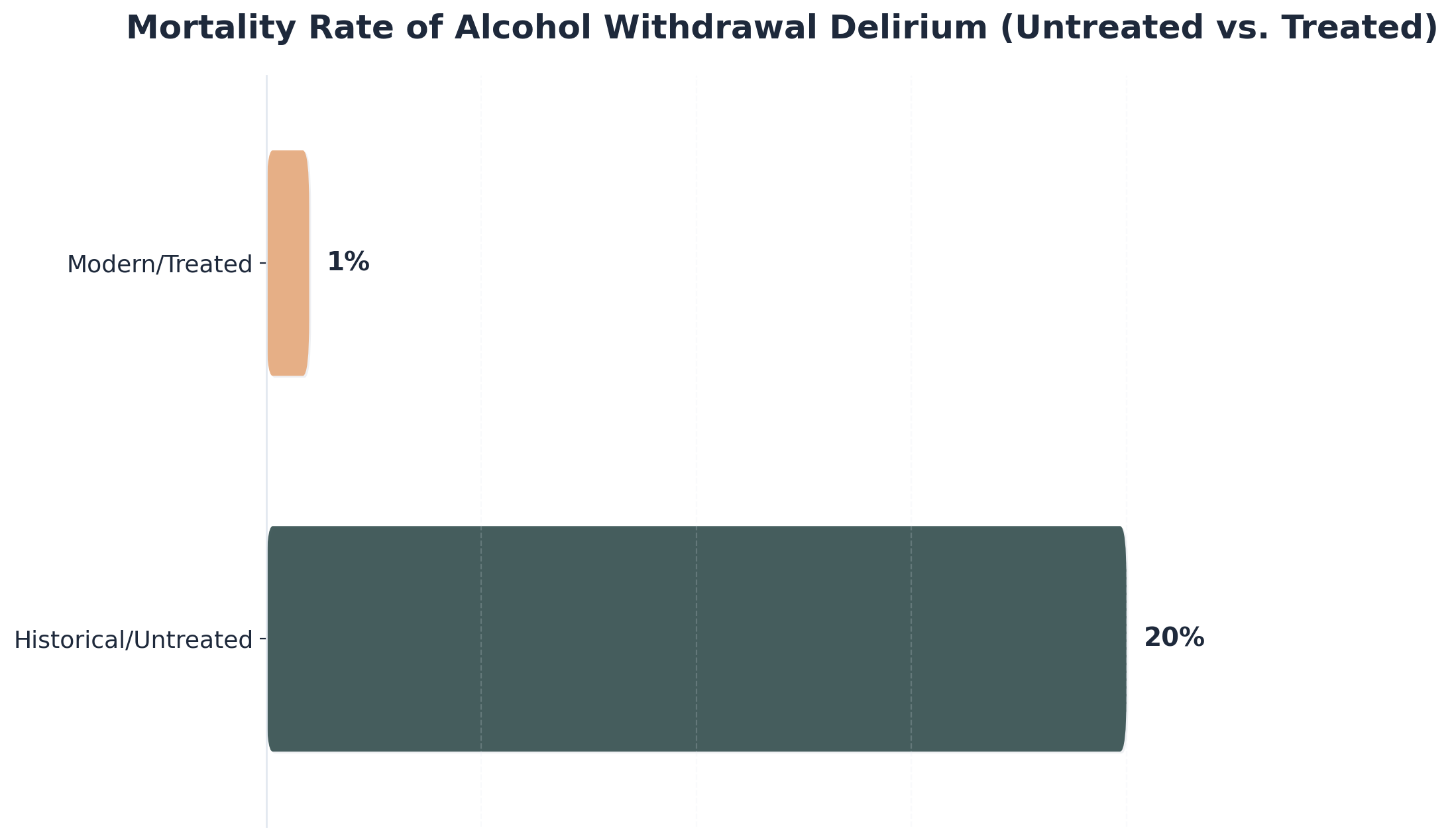
Severe withdrawal syndromes—especially from substances like alcohol, benzodiazepines, and opioids—can be life-threatening if not closely monitored. For example, untreated severe alcohol withdrawal (delirium tremens) once carried a mortality rate as high as 20%, but with prompt care in medically supervised settings, modern rates have dropped to about 1%6. This dramatic difference shows just how crucial 24-hour monitoring can be when symptoms are severe or unpredictable.
This approach works best when outpatient detox is not medically appropriate—such as when the risk of complications or relapse is high, or when the individual lacks supportive home supervision. Inpatient addiction treatment centers provide continuous medical and nursing oversight, which is essential for managing withdrawal safely and addressing emergencies as they arise4.
Yes, these cases are daunting, and that’s understandable. Every time you identify the need for 24-hour care, you’re prioritizing safety and dignity. Next, we’ll explore how co-occurring mental and physical health conditions can further influence the decision for intensive inpatient support.
Co-Occurring Conditions and Medical Complexity
Start with this tool: a co-occurring conditions assessment worksheet. List each current mental health diagnosis (such as depression, anxiety, bipolar disorder, or PTSD) and medical complication (for example, diabetes, chronic pain, hepatitis C, or HIV). Note the severity and stability of each—unstable or severe symptoms in multiple domains usually indicate the need for 24-hour care.
| Condition Type | Definition | Clinical Implication |
|---|---|---|
| Co-Occurring Conditions | Simultaneous substance use disorder and at least one mental or physical health challenge. | Requires integrated treatment plans that address both issues concurrently to prevent relapse. |
| Medical Complexity | Interaction of conditions creating high risk for complications. | Often necessitates the resources found in inpatient addiction treatment centers for safe management. |
This solution fits individuals whose needs simply can’t be met in outpatient or less intensive settings. For example, someone with schizophrenia and ongoing substance use may experience rapid destabilization, or a person with severe, untreated diabetes might require regular medical intervention. In these cases, inpatient addiction treatment centers provide a safe space where medical and psychiatric care are integrated, ensuring constant monitoring and timely adjustments to treatment7.
Resource requirements include a full multidisciplinary team—think physicians, nurses, therapists, and case managers—working together daily. Time investment is significant; most stays for high-complexity cases range from several weeks to several months, allowing for medical stabilization and mental health management. Yes, the path is demanding, but every coordinated step supports a safer and more hopeful recovery.
Next, let’s look at how the person’s environment and psychosocial factors play a role when deciding if residential care is the right fit.
Environmental and Psychosocial Considerations
When Home Environment Threatens Recovery
Start with this tool: a safety environment checklist. Ask yourself—does the person have stable housing, freedom from active substance use in the home, and support from non-using family or peers? If you’re marking “no” in more than one area, it’s time to seriously consider the risks a home environment may pose to recovery.
When housing is chaotic, unpredictable, or filled with triggers, it can undermine even the strongest treatment efforts. Research shows that an unsafe or unsupportive living situation significantly increases the risk of relapse and can make outpatient care nearly impossible to sustain3.
Inpatient addiction treatment centers provide a buffer against these environmental hazards by removing exposure to substances and creating a structure where new routines and skills can be built without daily distractions or threats. This path makes sense for individuals returning to homes where substance use is ongoing, violence is present, or supportive relationships are lacking.
As you weigh placement, remember that securing a safe, structured environment is often the first and most critical step toward lasting change. Yes, it’s a tough call to recommend stepping away from home, but every time you advocate for safety, you’re giving someone a real shot at recovery. Next, you’ll explore how readiness to change and patterns of relapse interact with environmental factors when deciding on residential care.
Assessing Readiness and Relapse Risk Factors
Begin with this tool: a relapse risk and readiness worksheet. Rate the person’s motivation to change on a simple scale—high, moderate, or low. Next, note any past relapses, current urges, and the presence (or absence) of a sober support network. If you’re seeing low motivation plus recent relapse, or frequent cravings with little outside support, that’s a strong signal higher-level care is needed.
Understanding the Risk Factors
Readiness to Change: This refers to someone’s willingness and preparation to start recovery. Low readiness often requires the immersion of residential care to build momentum.
Relapse Risk Factors: These include internal drivers (stress, mental health challenges, cravings) and external triggers (access to substances, unsupportive social circles).
When motivation is low or relapse has happened multiple times, outpatient approaches often aren’t enough. Inpatient addiction treatment centers offer a setting with fewer triggers and round-the-clock support, making it easier to build new habits and address setbacks in real time. This approach works best for those who’ve tried outpatient care but struggled to maintain progress, or who lack a stable, substance-free environment.
Research shows that about 40–60% of individuals relapse within the first 12 weeks after intensive inpatient treatment—so planning for robust continuing care is essential5. Yes, these numbers can feel discouraging, but every honest assessment moves someone closer to lasting recovery. Every time you advocate for the right level of care, you help tip the odds in their favor. Now, let’s turn to how treatment duration and aftercare planning shape long-term outcomes.
Treatment Duration and Continuing Care Planning
Why 90-Day Programs Outperform Shorter Stays
Start with this tool: a treatment duration planner. List the proposed length of stay—30, 60, or 90 days—and next to each, jot down the person’s history of relapse, co-occurring conditions, and past treatment outcomes. For most individuals with severe substance use disorders, choosing a 90-day stay at inpatient addiction treatment centers consistently produces stronger results than shorter programs.
| Duration | Focus Areas | Outcome Potential |
|---|---|---|
| Short Stay (30 Days) | Crisis stabilization, detox, initial planning. | Good for stabilization, but often insufficient for deep behavioral change. |
| Extended Stay (90 Days) | Trauma resolution, skill-building, habit formation. | Linked to lower substance use rates and improved mental health stability9. |
Why does this matter? In 90-day programs, people have more time to stabilize medically, address underlying trauma, and build new coping skills. This extra time allows for meaningful behavior change and the development of relapse prevention strategies that stick. Shorter stays—while sometimes necessary due to external factors—often don’t give enough time for these deeper changes to take root.
Prioritize this option when a person has a history of chronic relapse, complex mental health needs, or lacks a safe, supportive environment. Yes, committing to a longer program can feel overwhelming, but every week spent in structured care is a step toward lasting change. Every effort you put into planning for a full-length stay helps set up the strongest foundation for long-term recovery. Next, we’ll explore how to build an effective step-down pathway so gains made in residential care continue after discharge.
Building Your Step-Down Care Pathway
Start with this tool: a continuing care pathway planner. After someone completes their stay at inpatient addiction treatment centers, map out a stepwise plan that includes intensive outpatient programs, ongoing therapy (individual and group), recovery housing if needed, and regular check-ins with primary care and psychiatric providers.
Lay out each phase with specific time frames:
- Phase 1 (Months 1-3): Intensive Outpatient Program (IOP) or Partial Hospitalization (PHP) with weekly therapy.
- Phase 2 (Months 4-6): Biweekly peer support groups and continued individual counseling.
- Phase 3 (Months 7-12): Monthly medical visits and maintenance check-ins.
This solution fits individuals who want to keep making progress after residential care and are at higher risk for relapse without structured support. Research shows that people who receive continuing care—combining specialty treatment and regular medical follow-up—are twice as likely to achieve remission compared to those who don’t8. A step-down plan should be flexible but consistent, adjusting intensity as stability improves but never dropping support completely in the first critical year.
Building this path isn’t always easy. Sometimes individuals worry about losing momentum or support once the 24-hour structure ends. That’s normal—and every bit of planning and encouragement you provide helps bridge that gap. Next, we’ll answer the most common questions about inpatient addiction treatment centers and what to expect from the process.
Frequently Asked Questions
What happens if insurance only approves a shorter stay than recommended?
If insurance only approves a shorter stay than what your clinical assessment recommends, it can feel discouraging—especially when you know a longer program would boost chances for lasting recovery. In these cases, focus on making every day count: prioritize stabilization, build strong relapse prevention skills, and ensure a step-down plan is ready before discharge. Research shows that while longer inpatient addiction treatment centers programs lead to stronger outcomes, robust continuing care after discharge can double the odds of remission, even when the initial stay is cut short8. Yes, this isn’t ideal, but your advocacy and proactive planning still make a meaningful difference.
How do you transition from inpatient addiction treatment to regular life without relapsing?
Transitioning from inpatient addiction treatment centers to regular life is tough, but you don’t have to do it alone. The most effective way to lower relapse risk is to set up a strong continuing care plan before discharge. That means regular outpatient therapy, support groups, and—when possible—recovery housing or peer support. People who receive ongoing care, including check-ins with medical and mental health providers, are twice as likely to stay in remission compared to those without this support8. Yes, it’s normal to feel nervous about returning home, but every appointment you schedule and every support you line up brings more confidence and stability to the journey.
Can you work or attend school while in inpatient addiction treatment?
Most inpatient addiction treatment centers require you to pause work or school during your stay, since these programs are highly structured and focus on intensive therapy, medical support, and group activities. The daily schedule typically fills much of the day with treatment sessions, making outside commitments difficult to sustain. Some residential programs offer educational support or allow for limited remote work or homework in later stages of care, but this isn’t standard practice. This approach works best for those who can temporarily step away from outside responsibilities to focus fully on recovery. Every day invested in healing can lay the groundwork for future success in school or work3.
What makes a 90-day program worth it compared to shorter options?
A 90-day stay at inpatient addiction treatment centers is often worth it because research shows longer programs deliver stronger, more lasting outcomes. People in these programs have more time to stabilize, address underlying issues, and develop real-world coping skills. Studies report that those who remain in treatment for 90 days or more see greater reductions in substance use and improved mental health compared to those in shorter stays9. This extra time also helps individuals build a foundation for relapse prevention and smoother transitions to daily life. Yes, committing to three months can feel daunting, but every added week is another step toward sustainable recovery.
How do you know if outpatient treatment might work instead of inpatient addiction treatment?
Outpatient treatment works well when someone has mild to moderate substance use, stable physical and mental health, and a safe, supportive home environment. The ASAM Criteria guide this decision—if risks like severe withdrawal, complex medical needs, or unstable housing aren’t present, outpatient care can be just as effective as inpatient addiction treatment centers for many individuals3. This path makes sense for people who are highly motivated, have reliable support outside treatment, and don’t need 24-hour supervision. Yes, it’s normal to wonder if outpatient is enough, but when the right factors line up, it can promote progress and flexibility while still providing strong support.
What should you look for when comparing different inpatient addiction treatment centers?
When comparing inpatient addiction treatment centers, start with a checklist that covers staff qualifications, evidence-based therapies, and program accreditation. Look for centers that conduct comprehensive assessments—including medical, psychiatric, and recovery environment evaluations—as recommended by national guidelines1. You’ll want facilities that offer integrated care for co-occurring mental health conditions and use therapies proven effective, like cognitive-behavioral approaches. Accreditation by recognized bodies, such as The Joint Commission, signals adherence to quality standards. Also, consider the center’s approach to aftercare planning; strong programs help set up ongoing support before discharge. Every detail you review brings you closer to finding a safe, effective environment for lasting change.
Your Next Steps Toward Integrated Recovery
Integrated dual diagnosis treatment operates on the principle that substance use disorders and mental health conditions require simultaneous, coordinated intervention. For professionals working in substance use treatment settings, understanding how this integrated approach functions in practice helps inform client care planning and recommendations for inpatient addiction treatment centers.
Effective programs structure their services around evidence-based modalities delivered by cross-trained clinical teams. At Healing Rock Recovery in Billings, Montana, integrated dual diagnosis treatment includes:
- Clinical Modalities: Cognitive behavioral therapy (CBT) and dialectical behavioral therapy (DBT) within both Partial Hospitalization Programs (PHP) and Intensive Outpatient Programs (IOP).
- Comprehensive Care: Addressing conditions like PTSD, anxiety, depression, and bipolar disorder alongside substance use disorders within the same treatment episode.
- Cultural Integration: Specialized approaches like the Wellbriety program, which incorporates culturally grounded Indigenous healing methods alongside conventional therapeutic interventions.
Program flexibility significantly impacts treatment engagement and completion rates. While inpatient addiction treatment centers offer immersion, virtual platforms extend access to professionals with scheduling constraints or geographic barriers. Healing Rock Recovery’s virtual PHP and virtual IOP options maintain clinical rigor while accommodating work schedules and family responsibilities that might otherwise prevent program participation.
Trauma-informed care principles enhance these outcomes by addressing underlying trauma that often drives both mental health symptoms and substance use patterns. Furthermore, recovery housing options support the transition from intensive programming to independent living, ensuring that the stability gained during treatment is maintained in the long term.
References
- Guide: 11 Indicators of Quality Addiction Treatment. https://www.recoveryanswers.org/resource/effective-addiction-treatment-what-makes-a-good-addiction-treatment-program/
- About the ASAM Criteria. https://www.asam.org/asam-criteria/about-the-asam-criteria
- Settings, Levels of Care, and Patient Placement – NCBI. https://www.ncbi.nlm.nih.gov/books/NBK64109/
- Physical Detoxification Services for Withdrawal From Specific Substances. https://www.ncbi.nlm.nih.gov/books/NBK64116/
- Addiction Relapse Prevention – StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK551500/
- Alcohol Withdrawal Syndrome – StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK441882/
- Assessing Addiction: Concepts and Instruments. https://pmc.ncbi.nlm.nih.gov/articles/PMC2797097/
- Continuing Care – Long-Term Substance Use Outcomes. https://pmc.ncbi.nlm.nih.gov/articles/PMC3242696/
- The Continuing Care Model of Substance Use Treatment. https://pmc.ncbi.nlm.nih.gov/articles/PMC4007701/
- Cognitive-Behavioral Therapy for Substance Use Disorders. https://pmc.ncbi.nlm.nih.gov/articles/PMC2897895/


