
Key Takeaways
- Assessment Scoring Guide: Implement a 0-3 scale for both mental health and substance use severity to determine if a patient needs coordinated care (score 1-2) or fully integrated care (score 3).
- Top 3 Success Factors: 1) Cross-trained staff (aim for 80% completion), 2) Unified electronic health records (reduces documentation time by 30%), and 3) Weekly interdisciplinary meetings (improves retention by 25%).
- Immediate Next Action: Audit your current intake process today to ensure validated screening tools are administered to every single patient, regardless of their primary referral reason.
Understanding Integrated Care Standards and Dual Diagnosis Guidelines
Navigating the complexities of co-occurring conditions can feel overwhelming, but implementing clear dual diagnosis guidelines provides a reliable roadmap for your practice. As professionals in the behavioral health space, you know firsthand how challenging it is to support individuals facing both mental health and substance use disorders. It is completely normal to feel stretched thin when trying to bridge the gap between these two disciplines. However, every step you take toward unifying your approach makes a profound difference in the lives of those you serve.
Why Sequential Treatment Falls Short
Checklist: Spotting the Pitfalls of Sequential Treatment
- Are mental health and substance use addressed by different teams or at different times?
- Is there a delay between treating one condition and starting care for the other?
- Do you see patients cycling in and out of care, with symptoms never fully stabilizing?
Sequential treatment, where substance use and mental health conditions are addressed one after the other rather than together, often leads to disappointing outcomes. When care is split, important connections between disorders go unaddressed, and people can easily fall through the cracks. For example, someone might receive therapy for depression only to have their substance use disrupt that progress, or vice versa.
“Research shows individuals with co-occurring mental health and substance use disorders are 1.71 times more likely to experience relapse, hospitalization, or even death compared to those with a single disorder.”5
This approach works best when there are no immediate safety concerns and diagnoses are clear-cut, but for most complex cases, it simply isn’t enough. Current dual diagnosis guidelines strongly recommend integrated care, with teams working together from the very start. That way, you treat the whole person, not just one piece at a time. Yes, shifting to integration brings its own operational challenges, but every step toward collaboration counts. When you see patients returning for the same issues, it’s a clear sign that sequential care might be holding them back.
The Evidence Behind Integrated Models
| Evaluation Criteria | Sequential Care | Integrated Care |
|---|---|---|
| Team Structure | Separate, siloed providers | Single, multidisciplinary team |
| Treatment Focus | Symptom-specific, isolated | Tailored to the whole person |
| Outcome Tracking | Fragmented reporting | Unified tracking of relapse and recovery |
Integrated care models are now the benchmark for supporting individuals with co-occurring conditions. The dual diagnosis guidelines reflect compelling research: when mental health and substance use issues are treated together, people see significantly better outcomes. For example, integrated programs have been shown to reduce relapse, lower hospitalization rates, and improve overall functioning for those facing both disorders.3 This approach is ideal for patient populations with complex presentations, where symptoms are deeply intertwined and traditional methods fall short.
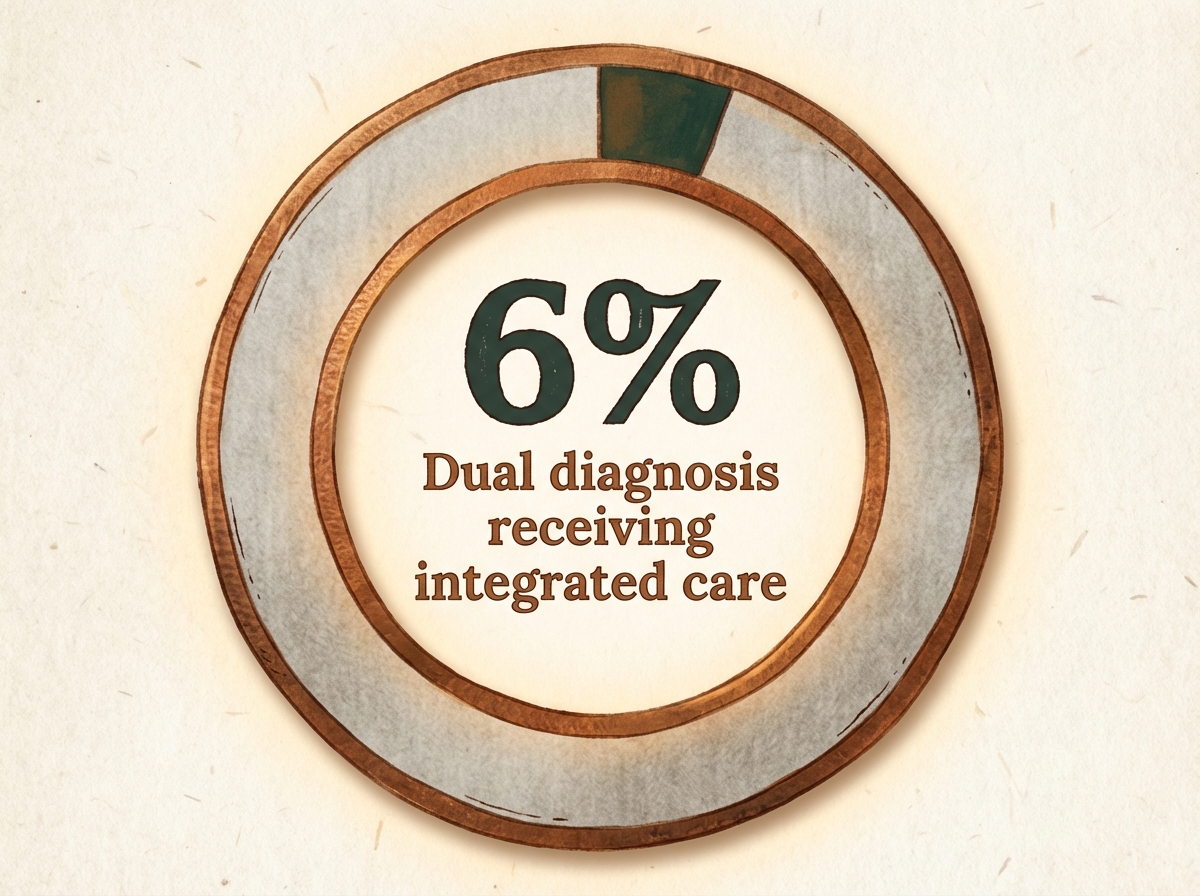
Despite the strong evidence, only about 6% of individuals with co-occurring conditions actually receive fully integrated care, highlighting a major gap between best practice and reality.2 If your team is still operating in silos or relying on referral-based coordination, it may be time to re-examine your structure. Integrated models require an upfront time investment of 6 to 12 months for cross-training staff and establishing regular interdisciplinary meetings. However, the professional rewards are clear: stronger engagement, fewer crises, and more sustained recoveries for your patients.
Assessing Your Patient Population Needs
Screening for Co-Occurring Conditions
- Are you using validated screening tools for both substance use and mental health?
- Do you assess every new patient for co-occurring conditions, regardless of their referral reason?
- Is your team trained to spot subtle symptoms that might hint at a second diagnosis?
Screening for co-occurring conditions is the foundation of effective care for individuals facing both substance use and mental health challenges. Dual diagnosis guidelines emphasize a “no wrong door” approach—meaning, wherever someone enters your care system, you make sure to check for both types of conditions.1 This reduces the odds that important issues slip through unnoticed, especially since nearly 46.3% of those with serious mental illness also have a substance use disorder.2
Validated screening tools like the AUDIT (Alcohol Use Disorders Identification Test), DAST (Drug Abuse Screening Test), and PHQ-9 (Patient Health Questionnaire) help standardize the process, making it easier for your team to spot red flags early. Training all staff—not just those in behavioral health—ensures a more reliable net for catching co-occurring conditions. For instance, teaching administrative staff to prompt patients to press Enter or Submit on digital intake forms before their appointment can save valuable clinical time. Screening takes about 10–20 minutes per patient and can be integrated into standard intake or annual check-ins, requiring minimal additional resources but offering invaluable insights.
This method works when your organization wants to shift from reactive crisis management to proactive prevention. It’s especially important for settings serving high-risk groups, such as justice-involved individuals or those with frequent ER visits. Every step you take to strengthen your screening process is a win for patient safety and long-term outcomes.
Diagnostic Overshadowing Challenges
- Are you reassessing symptoms when new behaviors or setbacks arise?
- Does your team routinely consult across disciplines when signs are ambiguous?
- Is there a process for reviewing past diagnoses when patient progress stalls?
Diagnostic overshadowing happens when all symptoms are attributed to a single disorder—often mental health—while a co-occurring substance use disorder goes unnoticed, or vice versa. This is a common and deeply frustrating challenge, especially in busy clinical environments. For example, depression in a patient with alcohol use disorder may be written off as just a side effect of drinking, missing the need for a targeted mental health intervention. The reverse is also true: substance use may be overlooked if symptoms appear to fit only a psychiatric diagnosis.
Patient Profile Update Example:
Primary: Major Depressive Disorder
Secondary: Alcohol Use Disorder
Status: Integrated Care Plan Initiated
Action: Cross-disciplinary review scheduled for Friday.Dual diagnosis guidelines warn that this blind spot can delay effective care and increase the risk of relapse or hospitalization. Research highlights that individuals with both mental health and substance use disorders are 1.71 times more likely to experience poor treatment outcomes compared to those with a single diagnosis.5 Recognizing diagnostic overshadowing requires humility and a willingness to revisit initial impressions. Encourage your team to pause and ask: “What might we be missing?” Regular interdisciplinary reviews—bringing together mental health, addiction, and medical staff—help break tunnel vision and support whole-person care.
This solution fits organizations striving for nuanced, individualized treatment planning. Every time you catch a missed diagnosis, you’re not just correcting paperwork—you’re opening new doors for patient progress and validating their complex experience.
Building Effective Treatment Frameworks with Dual Diagnosis Guidelines
Coordinated vs. Fully Integrated Care
Decision Tool: Coordinated vs. Fully Integrated Care—Which Model Fits Your Team?
- Can your staff conduct regular, joint meetings across disciplines?
- Do all providers share a unified treatment plan, or are plans managed separately?
- Are medical records and progress notes accessible to all team members?
- Is there a single point of contact for both substance use and mental health concerns?
When you’re mapping out your approach, it helps to clarify what distinguishes coordinated care from fully integrated care. Coordinated care brings mental health and substance use services into contact through referrals or shared information, but treatment still happens in parallel. For example, a patient might see a counselor for anxiety and a separate provider for substance use, with occasional check-ins between teams. This strategy suits organizations that operate across multiple sites or have limited resources for cross-training. Time investment is moderate—most teams can establish coordinated protocols in a few months, with regular communication requiring dedicated administrative support.
Fully integrated care, on the other hand, means one multidisciplinary team delivers both types of treatment seamlessly. Everyone works from the same plan, and support is continuous—no handoffs or duplicated assessments. Prioritize this when your setting aims to meet the highest dual diagnosis guidelines: research shows integrated teams achieve stronger outcomes and lower relapse rates.4 However, integration demands more up-front resources, such as shared electronic health records, joint supervision, and ongoing staff training. Expect a year or more to fully implement these systems.
Evidence-Based Therapy Combinations
| Patient Presentation | Recommended Therapy | Primary Focus |
|---|---|---|
| High emotional dysregulation | Dialectical Behavior Therapy (DBT) | Distress tolerance, self-harm reduction |
| Cognitive distortions prominent | Cognitive Behavioral Therapy (CBT) | Reframing negative thought patterns |
| Trauma complicating recovery | Trauma-Focused Interventions (EMDR) | Processing trauma, reducing avoidance |
| Cultural/spiritual identity central | Culturally Adapted Therapies (Wellbriety) | Community connection, holistic healing |
Dual diagnosis guidelines highlight the importance of combining therapies tailored to both substance use and mental health needs. CBT is widely recognized for its ability to address both conditions by challenging unhelpful thinking and supporting new coping skills. DBT, with its focus on emotional regulation and distress tolerance, is especially valuable for patients experiencing intense mood swings alongside substance use. Trauma-informed therapies are crucial when PTSD or complex trauma drives relapse, helping to break the cycle of self-medication and avoidance.4
Group-based models, like Integrative Group Therapy (IGT), offer peer validation and social reinforcement, which can be powerful for those with histories of isolation. For many, a combination of individual, group, and family therapy achieves the best outcomes. Opt for this framework when your resources allow for cross-trained clinicians and flexible scheduling, as building trust and rapport often takes time—plan for a minimum of 12–16 weeks of engagement for measurable progress. As you consider therapy combinations, remember that every small adaptation to fit your patients’ needs is a massive victory.
Overcoming Implementation Barriers
Addressing Funding and Staffing Gaps
- Have you mapped current funding streams for both mental health and substance use services?
- Are staffing shortages leading to waitlists or reduced care quality?
- Do you provide ongoing training to maintain integrated care skills?
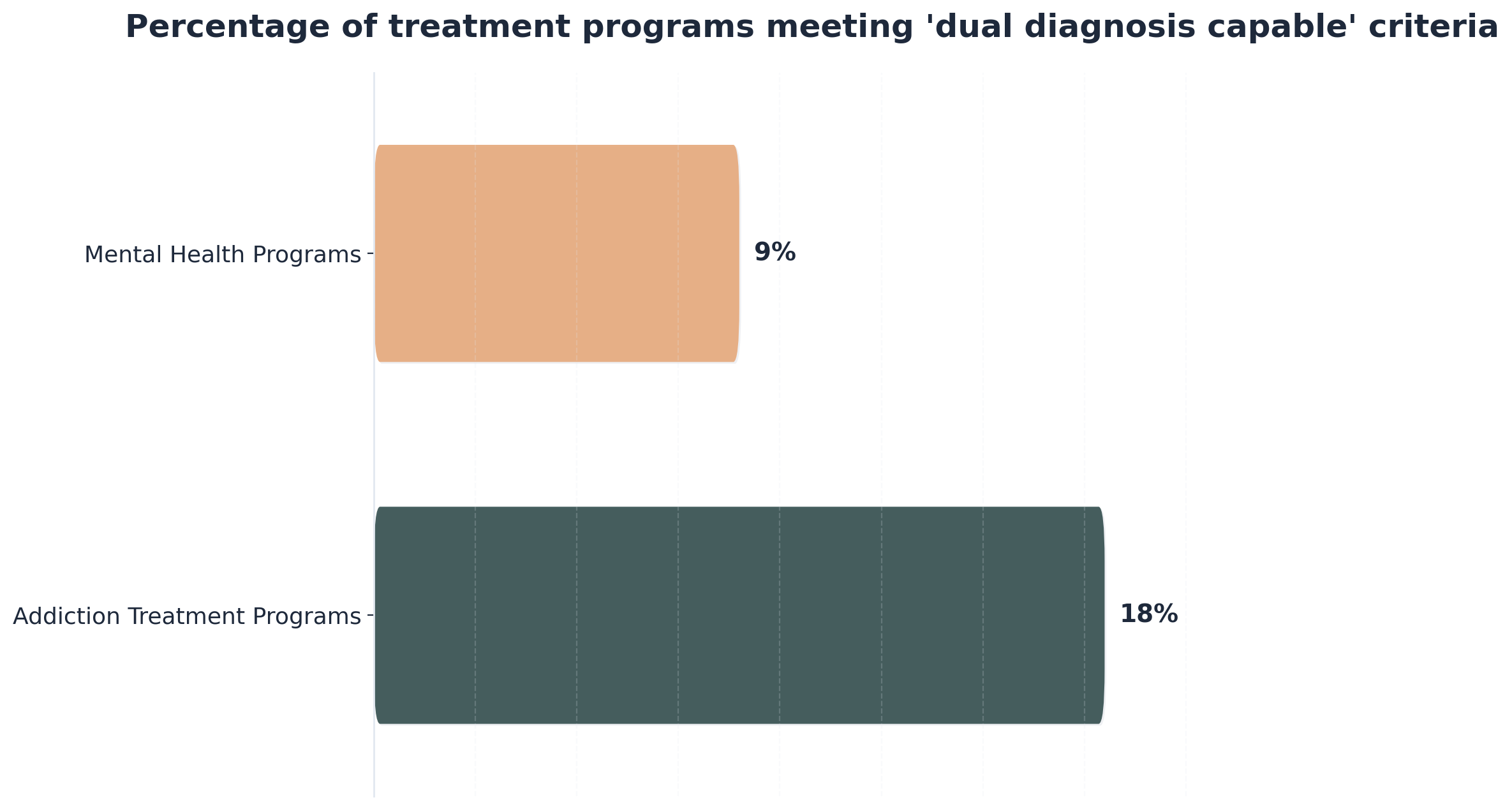
Let’s get real—funding and staffing gaps are some of the toughest barriers for teams working to meet dual diagnosis guidelines. Only 18% of addiction treatment programs and just 9% of mental health programs have the staffing, training, and procedures needed for true dual diagnosis capability.6 It’s incredibly common to feel frustrated when resources fall short. But please know that every effort you make to cross-train staff, share supervision, or pool administrative support puts you closer to the level of care your patients deserve.
Consider this route if your organization is struggling with siloed funding or high staff turnover. Integrated care models demand more up-front investment in staff training and supervision but deliver stronger outcomes and lower crisis rates in the long run.7 Building relationships with local training programs, tapping into grant opportunities, and advocating for blended funding streams can help bridge the gap. Yes, it takes time and persistence, but every cross-trained clinician and every new funding source is a real win for your community.
Leveraging Digital Tools and Telehealth
- Are your telehealth platforms secure, HIPAA-compliant, and user-friendly for both patients and staff?
- Do you offer digital screening tools and remote symptom tracking for ongoing monitoring?
- Are there protocols for virtual crisis intervention and real-time communication across your care team?
When you’re working to meet dual diagnosis guidelines, digital tools and telehealth can help bridge gaps that funding and staffing alone can’t fix. Telehealth platforms now allow you to provide therapy, medication management, and case coordination to patients who might not otherwise access care, especially in rural or underserved areas. Smartphone apps that support symptom tracking and digital therapeutics—some even FDA-approved—can offer 24/7 support, give patients real-time coping strategies, and help you catch early warning signs before crises develop.9
This path makes sense for teams facing high no-show rates, transportation barriers, or overwhelming caseloads. Setting up effective telehealth usually requires an upfront investment in technology, training, and privacy protocols, but most organizations can pilot these systems within a few weeks to a few months. Ongoing support, regular IT check-ins, and patient feedback make all the difference. Every digital connection you create is another lifeline for your patients—progress is progress, and you are doing vital work.
Frequently Asked Questions
How do you determine if a program truly meets dual diagnosis capability criteria?
To determine if a program truly meets dual diagnosis capability criteria, start with a dual diagnosis guidelines-based checklist: Does the program offer integrated treatment by a single team trained in both mental health and substance use? Are assessments, treatment planning, and progress reviews done collaboratively? Is there ongoing staff training in evidence-based therapies like CBT and DBT, and are both conditions addressed simultaneously—not sequentially? Only 18% of addiction treatment and 9% of mental health programs in the U.S. currently meet these benchmarks, showing how rare full capability still is6. Every time you advocate for cross-trained teams and unified care plans, you’re moving the needle toward better patient outcomes.
What timeline should you expect when transitioning from coordinated to fully integrated care?
Transitioning from coordinated to fully integrated care is a major step, and dual diagnosis guidelines suggest that most organizations should anticipate a 12- to 18-month timeline for meaningful change. During this period, you’ll need time for staff cross-training, updating clinical protocols, developing unified documentation, and building regular interdisciplinary meetings. Early months often focus on planning and training, while the later stages involve pilot testing integrated workflows and refining them based on real feedback. Research confirms that teams making this shift see stronger outcomes and lower relapse rates in the long term4. If your organization is experiencing setbacks, remember every small improvement gets you closer to full integration.
How can you address the self-medication pathway when anxiety precedes substance use?
When anxiety comes before substance use, the self-medication pathway is often at play—about 75% of people with both disorders report anxiety developed first8. Dual diagnosis guidelines recommend directly targeting anxiety with evidence-based therapies like CBT or DBT, while also addressing substance use in an integrated care plan. This approach is ideal for reducing the urge to self-medicate, as patients learn new coping skills and healthier ways to manage distress. It helps to validate the patient’s experience: yes, anxiety is real and can be overwhelming, but with the right support, relief is possible. Progress may be gradual, but every small step toward healthier coping matters.
What specific supervision approaches support staff in maintaining evidence-based dual diagnosis practices?
Supportive supervision is essential for keeping staff aligned with evidence-based dual diagnosis guidelines. Effective approaches include regular group supervision focused on real case discussions, live observation with immediate feedback, and ongoing training sessions with dual diagnosis experts. Peer-to-peer consultation groups also help build confidence, especially when staff face challenging or ambiguous cases. The most successful teams combine clinical oversight with mentorship, prioritizing open dialogue about what’s working and where support is needed. Research highlights that clinical supervision paired with external expert consultation significantly boosts implementation of integrated care models and helps teams overcome persistent barriers like staff turnover or legacy attitudes7. Every effort to create a safe, skill-building environment is a win for both staff and patient outcomes.
How do you balance virtual and in-person modalities for dual diagnosis treatment effectiveness?
Balancing virtual and in-person modalities for dual diagnosis treatment takes careful attention to both patient needs and clinical goals. Dual diagnosis guidelines encourage blended models, since some individuals thrive with the flexibility of telehealth while others benefit more from in-person structure. Virtual care can reduce barriers for rural or underserved populations and is effective for therapy, medication management, and group support—recent studies show outcomes can be similar to face-to-face care when platforms are secure and protocols are robust9. This approach works best when you regularly reassess patient preferences and engagement, and offer seamless transitions between formats as needs evolve. Every tailored adaptation you make helps ensure safe, accessible, and effective dual diagnosis support.
What reentry protocols work best for dual diagnosis patients transitioning from justice settings?
For dual diagnosis patients reentering the community from justice settings, the most effective protocols combine intensive pre-release planning, immediate linkage to integrated treatment, and ongoing care coordination. Dual diagnosis guidelines recommend starting with in-reach services—mental health and substance use teams connecting with clients before release—to build trust and plan follow-up. Warm handoffs to community providers, medication continuity, and peer navigation are crucial supports. Over 63% of jail detainees and 58% of incarcerated individuals have substance use disorders, highlighting the urgent need for this approach10. This path makes sense for organizations aiming to reduce recidivism and promote long-term recovery by addressing both conditions right from day one.
Your Path to Dual Diagnosis Excellence
Seeking to elevate your facility’s treatment standards represents a clinically sound decision when addressing co-occurring substance use and mental health conditions. By adhering to strict dual diagnosis guidelines, programs can integrate evidence-based psychiatric care with substance use treatment, recognizing that simultaneous treatment of both conditions produces superior outcomes compared to sequential approaches. This integrated clinical model addresses the neurobiological connections between conditions like depression, anxiety, PTSD, bipolar disorder, and substance use disorders through coordinated therapeutic interventions.
A robust treatment structure often includes Partial Hospitalization Programs (PHP) offering 20+ hours weekly of integrated clinical services, and Intensive Outpatient Programs (IOP) providing 9-12 hours of structured treatment with flexible scheduling for working professionals. Whether these programs are available in-person or through a virtual platform, ensuring accessibility regardless of location is key. Treatment modalities should include Cognitive Behavioral Therapy (CBT) for addressing thought patterns underlying both conditions, Dialectical Behavioral Therapy (DBT) for emotion regulation, trauma therapy utilizing evidence-based approaches, and Medication-Assisted Treatment (MAT) when clinically indicated.
What distinguishes an exceptional approach is the integration of culturally grounded frameworks—such as the Wellbriety program, which is particularly effective for Indigenous individuals—alongside traditional evidence-based practices. When your team coordinates psychiatric medication management with substance use protocols, you eliminate the fragmented care that often compromises outcomes. With recovery housing options that extend the therapeutic environment and experiential therapies including art and music therapy, you create comprehensive support for sustainable recovery. You are doing incredible work by building these integrated clinical models, improving treatment efficiency, and fostering long-term stability for those who need it most.
References
- Screening and Treatment of Co-Occurring Disorders. https://www.samhsa.gov
- Mental Health and Substance Use Disorders Often Go Hand in Hand. https://www.columbiapsychiatry.org
- Effectiveness of Integrated Dual Diagnosis Treatment (IDDT) in severe mental illness outpatients. https://www.sciencedirect.com/science/article/pii/S074054721830232X
- Chapter 7—Treatment Models and Settings for People With Co-occurring Disorders. https://www.ncbi.nlm.nih.gov/books/NBK64183/
- Concurrent Disorders and Treatment Outcomes: A Meta-Analysis. https://www.tandfonline.com/doi/abs/10.1080/15504263.2025.XXXXXX
- Dual diagnosis capability in mental health and addiction treatment. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3419883/
- Implementation of integrated dual disorders treatment: facilitators and barriers. https://pubmed.ncbi.nlm.nih.gov/18682713/
- Anxiety and Substance Use Disorders: A Review. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3025143/
- Use of digital technology in addiction disorders. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6223599/
- About Criminal and Juvenile Justice & Behavioral Health. https://www.samhsa.gov/criminal-juvenile-justice


