Key Takeaways
- Essential Prerequisites: Access to comprehensive medical records, collateral contacts, and validated dual diagnosis assessment tools.
- Step 1: Gather biopsychosocial information to build a complete clinical picture, including trauma history and safety checks.
- Step 2: Apply standardized instruments to evaluate the six dimensions of patient needs accurately.
- Step 3: Differentiate between primary mental health conditions and substance-induced symptoms through careful observation.
- Successful Outcome: By systematically applying these steps, you will confidently create accurate, integrated treatment plans that support lasting recovery for your patients.
Why Dual Diagnosis Assessment Tools Differ
Screening vs. Comprehensive Evaluation
You know the difference between screening and comprehensive evaluation is more than just a matter of time or paperwork—it’s about getting the full story. When you utilize dual diagnosis assessment tools right from the start, you move beyond a simple snapshot. Screening is a quick check, often using a short questionnaire. Its purpose is to answer one clear question: does this person show signs of possible mental health or substance use challenges that need further investigation? It’s like the front door—fast, focused, and meant to catch as many people as possible who may need more help.1
But when someone screens positive, it’s just the beginning. That’s where a comprehensive evaluation steps in. Here, you’re not only confirming the presence of symptoms, but looking for the root causes, identifying overlapping disorders, and understanding how substance use, mental health, trauma, and life circumstances all interact.
“Every detail matters because missing a diagnosis can mean missing a life-saving intervention. Yes, this process can feel overwhelming, but every thorough evaluation brings a patient one step closer to real recovery.”
The stakes are higher with co-occurring disorders. A rapid screen can be 90-96% accurate against full evaluations, but it can’t replace the depth you reach by digging into cognitive, behavioral, and social patterns.6 As you move deeper into the evaluation process, understanding the true scope of comorbidity becomes even more important.
The 50% Comorbidity Reality
Facing the 50% comorbidity rate head-on is both sobering and motivating. You know that when someone presents with substance use concerns, there’s a one-in-two chance they’re also managing a mental health disorder. This reality is not just a statistic—it’s a daily truth in clinical practice, and it changes the way you approach every assessment.
When you work with dual diagnosis assessment tools, you are not just checking boxes; you are actively searching for the invisible threads that tie substance use and mental health together. Missing a co-occurring disorder means missing the opportunity for truly effective care. The presence of both conditions often leads to more severe symptoms, higher relapse rates, and greater functional impairment compared to treating either disorder alone.3
It’s understandable if this feels like a lot to manage, but every time you accurately identify both issues, you help create a path toward better outcomes. These instruments make it possible to systematically uncover hidden diagnoses, track symptom interplay, and shape treatment that truly addresses the complexity of a patient’s life.
| Statistic | Impact on Practice |
|---|---|
| 50% of those with substance use have a mental health disorder3 | Assess for both every time |
| Co-occurring disorders worsen outcomes | Integrated treatment is essential |
| Missed diagnosis leads to poorer prognosis | Comprehensive assessment saves lives |
Step 1: Gather Biopsychosocial Information
Medical Records and Collateral Sources
You know that dual diagnosis assessment tools are only as effective as the information you collect. That’s why starting with medical records and collateral sources is so vital. Medical records provide a clear window into a person’s health history, revealing patterns of mental health symptoms, previous substance use treatments, and key medical events.
Often, these records fill in gaps the patient may not recall or feel ready to share. In fact, clinicians turn to medical records in about 70% of assessment sessions, while information from other mental health providers is accessed in 30% of cases.9 You can quickly search electronic health records using Ctrl + F to locate specific DSM-5 codes or past medication trials.
Collateral sources—such as family, caregivers, or previous treatment teams—bring in details that round out the picture. You may uncover critical context about fluctuations in mood, medication adherence, or relapse triggers. Sometimes, a loved one’s perspective helps validate or clarify what’s in the chart or what the patient describes. This can be especially important in situations where insight is limited or when substance use interferes with memory.
| Collateral Source | Frequency of Use (%) |
|---|---|
| Medical Records | 70 |
| Other Mental Health Providers | 30 |
Safety and Trauma History Assessment
Approaching safety and trauma history in your evaluation is about creating a space where honesty feels possible. You know how vital it is to check for immediate safety risks before moving any deeper. Begin with gentle, direct questions about current safety, and remember that your calm presence can make these difficult conversations less overwhelming for the person in front of you.
- Suicidality: Assess for active ideation, intent, and plan.
- Self-Harm: Check for non-suicidal self-injury behaviors.
- Harm to Others: Evaluate any potential risks to the community or family.
After safety, exploring trauma history is the next step. Many people seeking substance use treatment have lived through experiences that shaped their coping, trust, and beliefs about themselves. Trauma—including childhood adversity, loss, violence, or discrimination—may not always be shared willingly unless you ask in a respectful, nonjudgmental way.
Effective dual diagnosis assessment tools often include short trauma screens or structured interviews to support this process.10 Using these tools helps you avoid missing trauma that may be driving symptoms or relapse. It’s normal to feel the weight of these disclosures, but every time you identify trauma, you open the door for healing, not just symptom management.
Step 2: Apply Standardized Dual Diagnosis Assessment Tools
ASAM Criteria and Six-Dimension Framework
You’re probably familiar with the ASAM Criteria, but it’s worth pausing to appreciate just how central this six-dimension framework is to effective dual diagnosis assessment tools. The ASAM Criteria is not just a checklist—it’s a structured way to see the whole individual in context. Each of its six dimensions asks you to consider a different aspect of the person’s needs, from acute intoxication and withdrawal potential to readiness for change and recovery environment.2
This approach helps you avoid tunnel vision, making sure substance use and mental health aren’t treated in isolation. The updated ASAM Criteria, now in its fourth edition, goes further by weaving ‘readiness to change’ into all six dimensions and introducing a new focus on person-centered considerations. These updates push you to look beyond symptoms and diagnosis, encouraging deeper reflection on barriers, strengths, and social determinants of health.2
| ASAM Dimension | Focus Area |
|---|---|
| 1. Acute Intoxication/Withdrawal | Risk of withdrawal or overdose |
| 2. Biomedical Conditions | Physical health needs |
| 3. Emotional/Behavioral Conditions | Mental health and symptoms |
| 4. Readiness to Change | Motivation and engagement |
| 5. Relapse/Continued Use Potential | Triggers and relapse risk |
| 6. Recovery Environment | Home, family, social context |
ASI, PRISM, and Rapid Screening Options
When you want a clear, structured picture of both substance use and mental health symptoms, dual diagnosis assessment tools like the Addiction Severity Index (ASI) and the Psychiatric Research Interview for Substance and Mental Disorders (PRISM) are your go-to resources. The ASI is one of the most widely used instruments. It covers seven areas that matter most: medical, employment, alcohol and drug use, legal, family/social, and psychiatric status.
By working through these sections, you get a snapshot of the person’s current situation and how their challenges interconnect. This makes the ASI especially helpful for guiding integrated treatment plans and tracking change over time.1 PRISM takes a structured interview approach, designed specifically to distinguish between primary psychiatric disorders and those caused by substance use. This is essential when symptoms overlap or shift with substance use patterns, which happens often in dual diagnosis cases.7
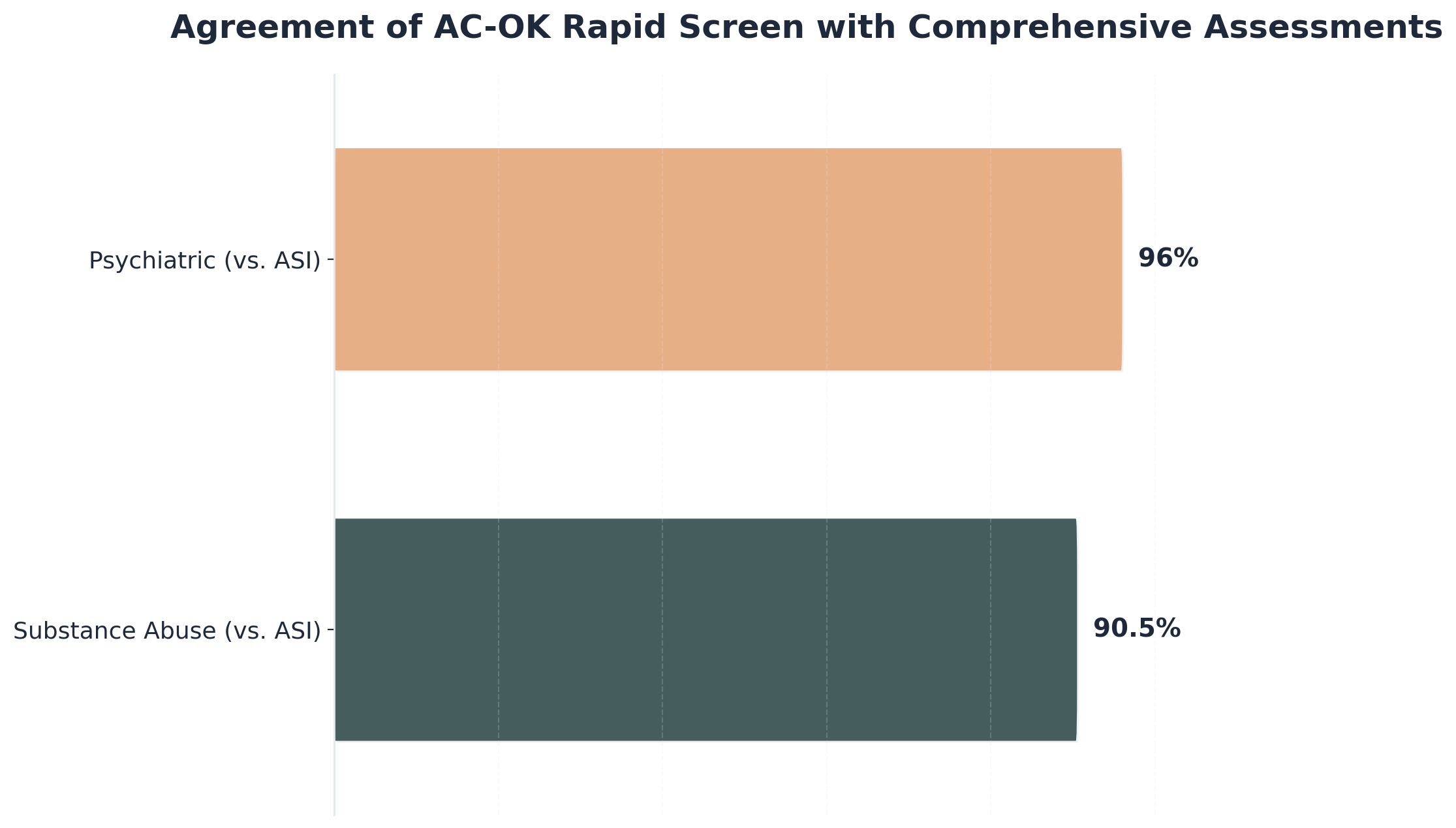
Rapid screening tools, such as the AC-OK Screen, help you catch possible co-occurring disorders in just a few minutes. The AC-OK has shown agreement rates of over 90% with the ASI for substance use and 96% for psychiatric concerns.6 This speed can feel like a relief when time is short, but remember: quick screens are a starting point, not a replacement for deeper assessment.
| Tool | Format | Strengths |
|---|---|---|
| ASI | Semi-structured | Broad overview; tracks change |
| PRISM | Structured | Distinguishes primary vs. induced disorders |
| AC-OK | Rapid screen | Fast; high agreement with ASI |

Step 3: Differentiate Primary vs. Induced
Understanding the difference between primary and induced mental health symptoms becomes crucial as you move forward in your clinical evaluations. This distinction helps shape your treatment approach and gives your patients realistic expectations about what healing will look like for them. Primary mental health conditions exist independently of substance use. These are conditions a patient might have experienced before they started using substances, or they would continue even with complete abstinence.
For example, if a patient struggled with anxiety attacks as a teenager before ever trying alcohol, that anxiety is likely a primary condition. Similarly, if depression runs in their family and they experienced symptoms long before substance use began, you’re dealing with a primary disorder. These conditions require ongoing treatment and management strategies that extend beyond addressing substance use alone.
Induced mental health symptoms, on the other hand, emerge directly from substance use or withdrawal. When patients use substances regularly, they alter their brain chemistry in ways that can mimic mental health disorders. Alcohol withdrawal commonly produces anxiety and depression. Stimulant use can trigger paranoia or psychotic symptoms. Opioid withdrawal often brings intense mood swings and emotional instability.
The key difference? These symptoms typically improve or resolve completely after a period of sustained abstinence and proper medical support. Here’s where things get tricky: the timeline matters significantly. Some induced symptoms clear up within days or weeks of stopping substance use. Others take months to fully resolve as the brain chemistry gradually rebalances.
View Timeline of Symptom Resolution
Understanding the timeline is essential when using dual diagnosis assessment tools. Acute withdrawal symptoms often peak within 3-7 days, while post-acute withdrawal syndrome (PAWS) can cause mood fluctuations for 6-18 months. Always reassess patients at multiple intervals to accurately differentiate primary from induced conditions.
This is why dual diagnosis treatment centers emphasize the importance of patience during early recovery. You might feel discouraged when a patient’s symptoms persist, but remember that their brain needs time to heal. Your treatment team uses several approaches to make this differentiation. You’ll review their personal history carefully, looking at when symptoms first appeared and how they’ve changed over time.
You’ll monitor how their symptoms respond to abstinence and treatment. If symptoms significantly improve after a few weeks of sobriety, they’re more likely induced. If they persist or existed before substance use, they’re probably primary conditions requiring specialized mental health treatment alongside recovery work. This distinction isn’t just academic—it directly impacts the treatment plan.
Frequently Asked Questions
What if a patient’s symptoms change significantly during the assessment period?
When a patient’s symptoms shift during assessment, it’s natural to feel uncertain. Remember, dual diagnosis assessment tools are designed to capture changes over time, not just a single moment. Fluctuating symptoms may signal the influence of substance use, withdrawal, or an evolving mental health condition. In these situations, keep ongoing communication open and document patterns as they emerge. Repeating key parts of the assessment after a period of stability can help clarify whether symptoms are primary or substance-induced 7. Trust that every observation you make during these changes brings you closer to an accurate diagnosis—progress, not perfection, is the goal.
How can clinicians overcome time constraints when implementing comprehensive dual diagnosis assessments?
Time constraints are a real challenge when you want to deliver thorough, compassionate care. Nearly half of clinical staff report lack of time as their biggest barrier to implementing comprehensive dual diagnosis assessments 8. To ease this strain, you can use brief, validated dual diagnosis assessment tools like rapid screens for initial triage, then return for deeper evaluation as time allows. Prioritizing high-risk cases and sharing assessment responsibilities across your team also helps reduce the load. Remember, even small steps—like scheduled reassessment or using structured tools—move you closer to safe, integrated care. Every bit of progress you make counts.
When should you reassess a dual diagnosis after the initial evaluation?
Reassessment of a dual diagnosis is best done whenever there’s a major clinical change, a new concern about safety, or a noticeable shift in symptoms or functioning. You might also want to reassess after a period of abstinence, as symptoms can look very different once substances clear from the system. Dual diagnosis assessment tools are meant for ongoing use, not just a one-time event—so schedule regular follow-ups, especially if the initial diagnosis was made during a crisis or withdrawal. Remember, consistent monitoring leads to more accurate diagnoses and better outcomes for your patients 1. Every time you check in, you’re supporting their journey toward lasting recovery.
What happens if collateral information contradicts the patient’s self-report during assessment?
When collateral information contradicts a patient’s self-report, it’s normal to feel stuck or even frustrated. Remember, dual diagnosis assessment tools are designed to bring together many perspectives for a deeper understanding. Contradictions can point to gaps in memory, denial, shame, or even misunderstandings between sources. Instead of choosing one side, create space for discussion—gently explore inconsistencies with the patient, and validate that it’s okay for stories to differ. Document each version and use your clinical judgment, drawing on collateral sources and your relationship with the patient to clarify the most likely scenario 9. Every honest conversation builds trust and brings you closer to the truth.
Can rapid screening tools like AC-OK replace comprehensive assessments in certain situations?
Rapid screening tools like AC-OK can be a valuable first step, especially when time or resources are limited. These tools are shown to have high agreement rates—over 90% for substance use and 96% for psychiatric symptoms compared to comprehensive assessments like the ASI 6. But remember, even the best rapid dual diagnosis assessment tools are not a substitute for a thorough evaluation. They can help you quickly identify those who need deeper assessment, but they may miss complex symptoms, trauma, or less obvious co-occurring disorders. When possible, use rapid screens to guide further steps—not as the final word. Every quick screen is progress, but a full assessment is still essential for safe, integrated care.
How do cultural factors influence dual diagnosis assessment accuracy?
Cultural factors play a powerful role in the accuracy of dual diagnosis assessment tools. If you overlook someone’s cultural background, language, or belief systems, you might misinterpret symptoms or miss key risk and protective factors. For example, expressions of distress or coping styles can look very different across cultures. Some communities may underreport symptoms due to stigma or mistrust of mental health systems. Even standardized tools can lose accuracy if they aren’t adapted for the person’s language or lived experience 1. The best practice is to approach every assessment with cultural humility—ask questions, listen deeply, and remember that every detail you learn about a person’s culture brings you closer to an accurate, respectful evaluation.
Conclusion
Understanding the difference between primary and induced mental health symptoms is a crucial step in the recovery journey. When you can recognize which symptoms stem from substance use and which existed before, you’re better equipped to work with your treatment team on a plan that addresses unique needs. This knowledge empowers you to make informed decisions about care and helps you understand why certain symptoms may improve as patients progress through treatment.
Remember, you don’t have to figure this out alone. As a qualified professional, you use comprehensive dual diagnosis assessment tools, observation over time, and evidence-based approaches to help distinguish between primary and induced conditions. This process takes patience, but it’s worth it. Getting an accurate dual diagnosis means your patients will receive targeted therapies that address both their mental health and substance use concerns simultaneously.
Every person’s path to recovery looks different, and that’s completely okay. By taking time to understand their symptoms and working diligently as an experienced clinician, you’re investing in a foundation for lasting healing and wellness. You are doing incredible work, and every accurate assessment changes a life.
References
- Chapter 3—Screening and Assessment of Co-Occurring Disorders. https://www.ncbi.nlm.nih.gov/sites/books/NBK571017/
- The ASAM Criteria. https://www.asam.org/asam-criteria
- Assessment of clinical co-morbidities. https://pmc.ncbi.nlm.nih.gov/articles/PMC5844155/
- Integrated Treatment of Substance Use and Psychiatric Disorders. https://pmc.ncbi.nlm.nih.gov/articles/PMC3753025/
- PTSD Checklist for DSM-5 (PCL-5). https://www.ptsd.va.gov/professional/assessment/adult-sr/ptsd-checklist.asp
- The AC-OK Screen for Co-Occurring Disorders. https://ccsme.org/wp-content/uploads/2017/02/AC-OK-Screening-tool.pdf
- Psychiatric Research Interview for Substance and Mental Disorders. https://pubmed.ncbi.nlm.nih.gov/8780425/
- Counselor Assessments of Training and Adoption Barriers. https://pmc.ncbi.nlm.nih.gov/articles/PMC1989156/
- Measuring and Quantifying Collateral Information in Psychiatry. https://pmc.ncbi.nlm.nih.gov/articles/PMC8082386/
- Screening and Assessment – Trauma-Informed Care in Behavioral Health. https://www.ncbi.nlm.nih.gov/books/NBK207188/