
Key Takeaways for Treatment Professionals
- Assess Acuity Accurately: Utilize the provided risk gauge to determine when inpatient mental health treatment centers are the absolute necessary level of care versus when PHP/IOP is viable.
- Navigate Capacity Constraints: With occupancy rates at 118%, understand the strategic importance of discharge planning starting at admission to prevent bottlenecks.
- Prioritize Continuity: Bridge the gap where 40% of patients fail to receive follow-up care by coordinating warm handoffs to step-down programs like Healing Rock Recovery.
Understanding Inpatient Mental Health Treatment Centers
What Defines Inpatient Mental Health Treatment
inpatient mental health treatment centers represent the highest level of care for people experiencing severe psychiatric distress. At its core, inpatient treatment means a person stays in a hospital or psychiatric facility, receiving round-the-clock support to manage risks that simply cannot be handled in an outpatient setting. Acute symptoms—like suicidal thoughts, aggressive outbursts, or an inability to perform basic self-care—are typical reasons someone might require this level of intervention.
To ensure you are correctly identifying this level of care, consider the following core elements:
- 24/7 Clinical Supervision: Continuous monitoring in a secure environment.
- Physician-Led Care: Daily psychiatric assessments and immediate medication management.
- Intensive Intervention: Daily therapeutic modalities including individual, group, and family sessions.
- Acute Stabilization: A primary focus on safety and symptom reduction rather than long-term therapy.
- Structured Routine: Strict monitoring of basic needs and daily schedules.
These centers are designed for short-term crisis stabilization. You will see intensive therapy, constant monitoring, and a highly structured environment. Medical teams, including psychiatrists, nurses, and therapists, coordinate efforts to help stabilize symptoms and lay the groundwork for ongoing recovery. For many, the goal is to get through a crisis period safely, then step down to less restrictive care when appropriate.
“This approach works best when someone’s safety or judgment is so impaired that home or community programs would not be enough. Inpatient mental health treatment centers also provide a crucial setting for medication adjustments and observation that can’t be done safely elsewhere10.”
Yes, this is challenging work, and it is important to recognize every small milestone as progress on the path to stability. Next, we will look at the growing crisis in psychiatric bed access and what it means for those who need this essential level of care.
The Current Crisis in Psychiatric Bed Access
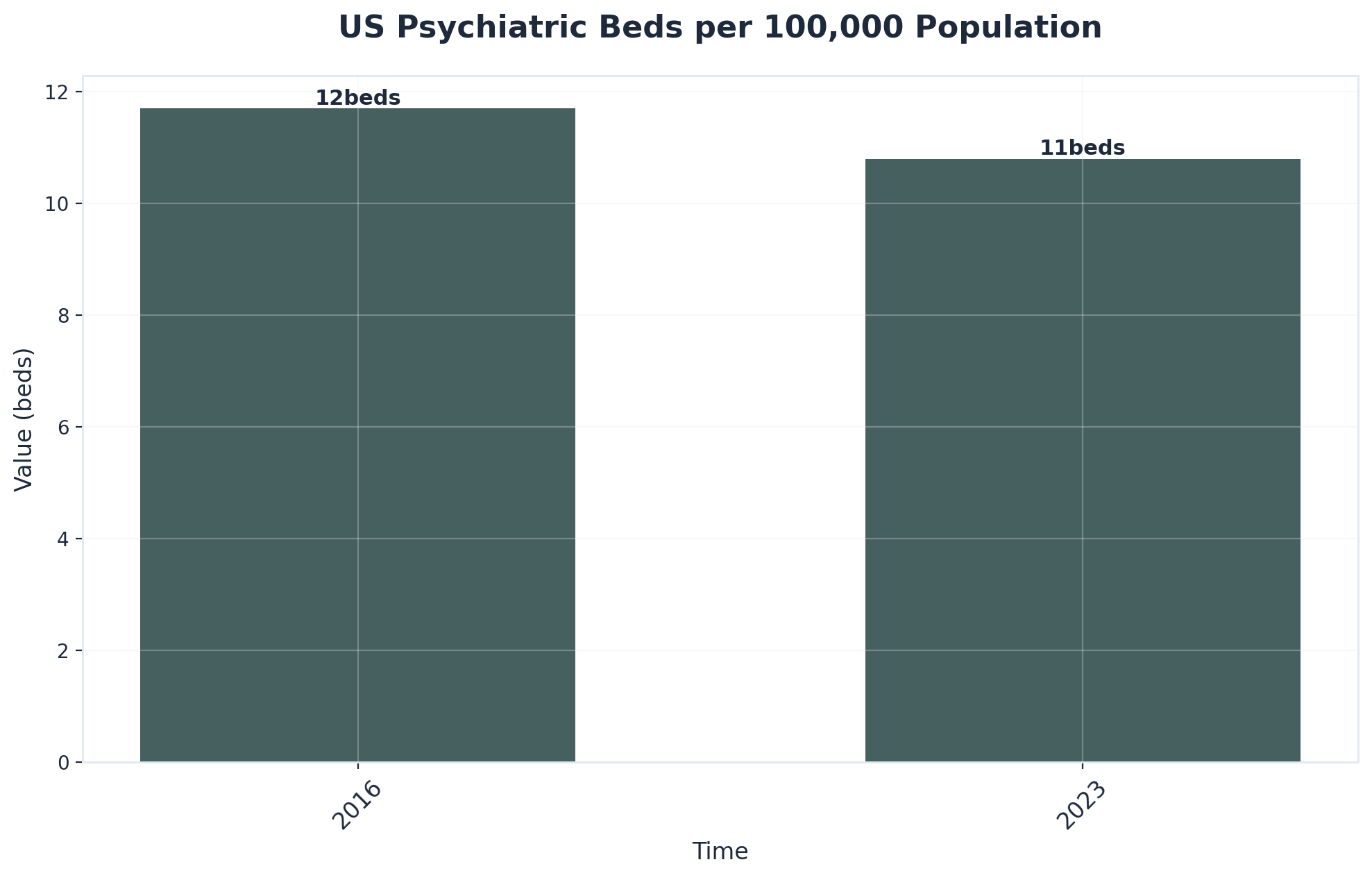
Across the country, inpatient mental health treatment centers are under immense pressure. The number of available psychiatric beds has dropped to just 10.8 per 100,000 people—a continued decline since 20161. As a result, utilization rates have soared far above thresholds considered safe for quality care.
| Metric | Recommended Standard | Current Reality (2018 Data) |
|---|---|---|
| Occupancy Rate | 85% (Safe Capacity) | 118% (Over Capacity)6 |
| Bed Availability | 40-60 per 100,000 | 10.8 per 100,0001 |
| Staffing Status | Full Clinical Teams | 94% of state hospitals report shortages6 |
If you are evaluating the strain on your local resources, use this risk gauge to assess the severity in your community:
- Are emergency departments in your region regularly boarding psychiatric patients?
- Do you routinely face delays of 24+ hours to secure an inpatient bed?
- Are more than half of state psychiatric beds occupied by forensic or court-involved patients?
- Are local inpatient mental health treatment centers operating above recommended occupancy rates?
- Have you observed an uptick in staff burnout or turnover linked to resource strain?
If you answered “yes” to several of these, your community is likely experiencing the current psychiatric bed crisis. When resources are this stretched, it is easy to feel discouraged. Still, every effort to advocate for a patient or support a colleague matters—progress is possible, even in small steps.
Clinical Indicators for Admission to Inpatient Mental Health Treatment Centers
Acute Safety Risks and Crisis Situations
Acute safety risks stand out as the most urgent reason for choosing inpatient mental health treatment centers. These facilities are designed to address situations where someone’s life or the safety of others is at immediate risk. Suicidal ideation, recent suicide attempts, or clear plans for self-harm all signal the need for 24/7 monitoring.

Use the following decision tool to determine if acute safety risks require immediate admission:
- Suicidality: Is there evidence of suicidal intent, a recent attempt, or ongoing thoughts with a specific plan?
- Violence: Has the person expressed or acted on threats of violence toward others?
- Psychosis: Are psychotic symptoms (hallucinations, delusions) causing behaviors that put the person or others in immediate danger?
- Self-Neglect: Is self-care so impaired that basic needs—like eating, hygiene, or shelter—are neglected to a life-threatening degree?
- Escalation: Has the current crisis escalated beyond what outpatient or community resources can safely address?
If you answer “yes” to any of these, it is time to prioritize inpatient admission for stabilization. This approach works best when judgment is so impaired that less intensive settings would put everyone at risk. In these moments, the presence of trained staff and continuous observation is not just best practice—it is a life-saving intervention.
Click to view clinical necessity criteria
Research confirms that admission is medically necessary whenever acute danger to self or others is present, or when basic functioning collapses to the point where outpatient care is unsafe or ineffective10. Responding quickly in these scenarios is tough and emotionally taxing—but every action you take can prevent tragedy and offer a critical turning point for recovery.
Severe Functional Impairment and Co-Occurring Disorders
Severe functional impairment means a person is unable to carry out basic daily activities or maintain relationships, work, or self-care. When this impairment is paired with a co-occurring disorder—meaning both mental health and substance use disorders are present—the complexity of care skyrockets. Roughly 46% of people with a primary mental health or substance use diagnosis also live with a co-occurring condition4.
Consider inpatient mental health treatment centers if the following conditions are met:
- Does the individual struggle with both a mental health disorder and a substance use disorder (dual diagnosis)?
- Are daily living skills—like feeding, bathing, or maintaining housing—significantly compromised?
- Is there ongoing, severe mood instability, psychosis, or cognitive impairment that prevents safe community living?
- Have previous outpatient or step-down programs failed to prevent repeated crises?
- Is there a history of medical complications related to substance use or psychiatric symptoms?
These cases often require the intensive, coordinated approach only inpatient settings can deliver. This strategy suits organizations working with patients who cycle through repeated hospitalizations or have not responded to lower levels of care. For dual diagnosis cases, simultaneous treatment of both conditions is critical to break the cycle of relapse and crisis4.
Populations Most Likely to Require Inpatient Care
Understanding which populations benefit most from inpatient-level care helps treatment professionals make appropriate referral decisions and level-of-care determinations. Inpatient mental health treatment centers provide 24/7 medical supervision and structured therapeutic environments for patients facing the most acute recovery challenges. While Healing Rock Recovery specializes in Partial Hospitalization Programs (PHP) and Intensive Outpatient Programs (IOP), recognizing when patients require higher levels of care remains essential for effective treatment matching.

| Population | Clinical Necessity for Inpatient | Step-Down Opportunity (PHP/IOP) |
|---|---|---|
| Severe Withdrawal | Requires medical supervision for detoxification from alcohol, benzodiazepines, or opioids to manage life-threatening complications. | Post-stabilization transition to PHP for continued therapeutic support once medical risks subside. |
| Dual Diagnosis | Acute psychiatric crises combined with substance use may require stabilization in a secure environment. | Integrated treatment at centers like Healing Rock Recovery allows for comprehensive care in a less restrictive setting. |
| Treatment Resistant | Patients with multiple failed treatment episodes may need the rigid structure of inpatient care to break the cycle. | Well-structured PHP can provide daily engagement and skills practice in a real-world environment. |
| Unstable Housing | Lack of safe environment may necessitate inpatient care to ensure safety during early recovery. | Recovery housing combined with PHP/IOP offers environmental stability without full hospitalization. |
| Chronic Pain | Complex medication management during withdrawal often requires 24/7 oversight. | Medically assisted treatment (MAT) in PHP can effectively manage pain and recovery simultaneously. |
| High-Risk Pregnancy | Severe substance use combined with obstetric risks may require inpatient monitoring. | Prenatal care coordination is often successfully managed through PHP with close obstetric communication. |
| Active Suicidality | Immediate safety assessment and stabilization are required for active ideation or recent attempts. | Transition to IOP/PHP is critical for ongoing support once the acute crisis has stabilized. |
Navigating the Continuum of Care Effectively
When Less Restrictive Options Are Appropriate
Less restrictive options include outpatient therapy, intensive outpatient programs, partial hospitalization, and community-based supports. These paths honor an individual’s autonomy and can be less disruptive for families and work life. Consider this route if a person’s symptoms are under control, safety can be maintained, and the home environment is supportive.
Use this decision tree to determine if alternatives to inpatient mental health treatment centers are appropriate:
- Is the person medically and psychiatrically stable?
- Can safety be managed with outpatient or intensive outpatient services?
- Is there strong family or community support available?
- Has the individual responded well to step-down care in the past?
- Are there no signs of imminent risk to self or others?
If you answered “yes” to most of these, exploring less restrictive alternatives may be appropriate. The majority of people living with mental health needs are safely and effectively treated in these settings when symptoms are not severe or crisis-level10.
“Opting for less restrictive care is not a sign of failure or ‘not doing enough’—it’s a strength-based approach that respects progress and empowers independence.”
Every time you help someone transition to a lower level of care, you are supporting their recovery journey and helping to preserve limited inpatient resources for those in acute crisis.
Planning for Successful Discharge and Continuity
Ensuring a smooth transition from inpatient mental health treatment centers to community-based care is a process that starts early. Building a strong discharge plan means you are not just sending someone out the door—you are giving them a roadmap for success. This approach is ideal when your goal is to prevent readmission and support ongoing recovery.
Follow this checklist to ensure continuity of care:
- Start Early: Begin discharge planning at admission, not just at the end.
- Secure Appointments: Schedule an outpatient follow-up appointment before discharge.
- Manage Meds: Coordinate medication management, including prescriptions and education.
- Engage Support: Involve family or support systems in the transition plan.
- Plan for Safety: Share crisis and relapse safety plans with all care team members.
- Connect Resources: Confirm access to community supports (housing, employment, peer groups).
Research shows that over 40% of individuals discharged from inpatient mental health treatment centers do not receive outpatient follow-up within 30 days, which can increase the risk of relapse or crisis6. Involving loved ones, social services, and outpatient providers in the planning process helps bridge gaps and keep momentum going. Every effort you make to confirm follow-up appointments or connect someone to resources counts, even if it feels like a small step9.
Frequently Asked Questions
What happens when all psychiatric beds in your area are full?
When all psychiatric beds in your area are full, emergency departments often become holding areas for people in crisis, sometimes for days at a time. This practice, known as “boarding,” can be tough for both patients and professionals—emergency rooms aren’t designed for ongoing psychiatric care, and the overstimulation can worsen symptoms. Inpatient mental health treatment centers are stretched thin, with 90% of states now reporting bed shortages and occupancy rates reaching 118% of safe capacity 6. During these times, every creative solution matters, from expediting discharges to seeking transfer options in other regions. Even when resources feel stretched to the limit, every effort to advocate for timely care helps keep hope alive for those waiting.
How long does the average inpatient mental health treatment stay last?
The average stay at inpatient mental health treatment centers usually ranges from 7 to 14 days, though this can vary depending on the severity of symptoms and individual treatment response. Short-term admissions are most common, focusing on crisis stabilization, medication adjustments, and safety planning. Some individuals with complex needs or slower symptom improvement may require longer stays, but the overall trend is toward shorter hospitalizations to help more people access limited beds. Over 40% of patients discharged from these centers do not receive outpatient follow-up within 30 days—making strong discharge planning especially important for lasting recovery 6.
What are the main differences between state psychiatric hospitals and private inpatient facilities?
State psychiatric hospitals are typically government-funded and focus on serving individuals with severe, persistent mental illnesses or those involved with the criminal justice system. In fact, over half of state psychiatric beds are now occupied by forensic patients, which limits access for others in crisis 5. Private inpatient facilities, on the other hand, are usually funded by insurance or out-of-pocket payments and tend to offer shorter stays, more amenities, and sometimes a broader range of therapies. While state hospitals often handle the most acute or complex cases, private centers can provide a more comfortable setting but may have stricter admission criteria. Each type of facility plays a unique role in the inpatient mental health treatment centers landscape, supporting different needs across the continuum.
Can someone refuse inpatient mental health treatment if they don’t believe they need it?
In most cases, adults can refuse admission to inpatient mental health treatment centers if they do not believe they need it—unless they meet criteria for involuntary commitment. Involuntary commitment laws allow someone to be hospitalized against their will when they are found to be a danger to themselves or others, or unable to care for their basic needs due to mental illness. This process is court-ordered and requires clear clinical evidence. While it can be distressing for patients and families, involuntary treatment is intended as a last resort when safety is at risk 7. Supporting autonomy and shared decision-making is always ideal, but sometimes urgent intervention is necessary for crisis stabilization.
What percentage of individuals actually receive follow-up care after inpatient discharge?
Research shows that just under 60% of individuals discharged from inpatient mental health treatment centers actually receive any follow-up care within the first 30 days. That means more than 40% leave these settings without timely connections to outpatient support, increasing their risk for relapse or crisis 6. For professionals, this gap can be discouraging—especially given how important continuity is for long-term recovery. If you’ve ever felt frustrated by missed connections or fragmented care, you’re not alone. Every successful follow-up appointment or outreach is a win worth celebrating, even when progress is gradual.
Why are emergency departments increasingly holding psychiatric patients instead of transferring them?
Emergency departments are increasingly holding psychiatric patients—often called “boarding”—because inpatient mental health treatment centers face severe bed shortages and staffing crises. With the number of psychiatric beds dropping to just 10.8 per 100,000 people and hospitals running at 118% of recommended capacity, there simply aren’t enough safe placements available 6. Many facilities are unable to admit new patients, especially when over half of state beds are reserved for forensic cases. This leaves emergency rooms as the only immediate option, even though they aren’t designed to provide therapeutic care. It’s a tough situation, and every effort to support patients during these waits is meaningful progress.
Conclusion
Understanding who typically needs inpatient care provides valuable context for treatment matching and level-of-care decisions. While acute medical stabilization remains essential for certain populations—particularly those facing severe withdrawal, active suicidal ideation, or medical complications requiring 24-hour monitoring—clinical outcomes research increasingly demonstrates that many individuals can achieve successful recovery through structured PHP and IOP settings. This is particularly true when integrated dual diagnosis treatment addresses co-occurring mental health conditions alongside substance use disorders.
The continuum of care offers multiple pathways to recovery, and effective treatment matching considers not just acuity but also therapeutic readiness, support systems, and specific clinical needs. For individuals who have completed medical detoxification or inpatient stabilization, step-down programs provide critical continuity while allowing gradual reintegration into daily responsibilities. Similarly, those whose clinical presentation does not require round-the-clock medical supervision often benefit from the intensive therapeutic structure of PHP or IOP without the disruption of residential placement. Flexible delivery models—including virtual programming—expand access for rural populations and working professionals while maintaining clinical rigor.
At Healing Rock Recovery, our dual diagnosis expertise, culturally-informed approaches including the Wellbriety program, and flexible in-person and virtual treatment options position us to serve diverse populations across the care continuum. Whether you are coordinating step-down care following inpatient stabilization or seeking appropriate PHP/IOP placement for clients with co-occurring disorders, we welcome professional consultation to discuss treatment matching and referral coordination. Our clinical team is available to collaborate on individualized care planning that aligns with your clients’ specific needs and recovery goals.
References
- Estimating Psychiatric Bed Shortages in the US. https://doi.org/10.1001/jamapsychiatry.2021.4245
- Mental Health Treatment Need and Treatment System Capacity. https://aspe.hhs.gov/reports/mental-health-treatment-need-treatment-system-capacity
- Chapter 1—Introduction to Substance Use Disorder Treatment. https://www.ncbi.nlm.nih.gov/books/NBK573400/
- Dual Diagnosis Capability in Mental Health and Addiction Treatment. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4065612/
- Use of State Psychiatric Hospitals, 2025. https://www.nri-inc.org/media/2526/tb-use-of-state-psychiatric-hospitals-2025.pdf
- Psychiatric Bed Shortages Reach Crisis Levels. https://bhbusiness.com/2024/01/23/exclusive-psychiatric-bed-shortages-reach-crisis-levels-as-demand-for-behavioral-health-care-skyrockets/
- Involuntary Commitment: What It Is, How It Works & Criteria. https://my.clevelandclinic.org/health/treatments/24942-involuntary-commitment
- Readmission of Patients to Acute Psychiatric Hospitals. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4289196/
- Effectiveness of Discharge Planning for Psychiatric Inpatients. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3653240/
- Guidelines for acute inpatient psychiatric treatment review. https://doi.org/10.1016/0163-8343(89)90099-2


